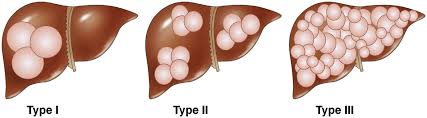
polycystic liver disease (PLD) is a rare hereditary disease. It presents in two forms: in isolation, in which patients have cysts only in the liver, and as an accompanying symptom of polycystic kidney disease (PKD), in which patients have cysts in both the liver and the kidney. Most cases of PLD occur as an accompanying symptom of PKD. In these patients, the kidney component typically dominates the clinical picture due to the development of renal failure and the need for dialysis or kidney transplantation. In contrast, isolated PLD is significantly more infrequent and rarely requires treatment. Although caused by different gene mutations, both forms of the disease are genetically determined and characterized by progressive development and enlargement of fluid-filled epithelial cysts throughout all segments of the liver. PLD diagnosis is typically made when the number of liver cysts exceeds 20. As a hereditary disorder, the leading risk factor for developing the condition is a family history of the disease. Generally, if one family member has PLD, the screening is recommended for all family members. Interestingly, women are more susceptible to developing a massive PLD compared to men who have the same genetic mutation. Although the precise reason for this is unknown, it is believed that female hormones may influence the growth of liver cysts. LIVER TRV45
Results of multiple studies support this theory by demonstrating that massive PLD is associated with pregnancy and exposure to exogenous sources of female hormones such as birth control or hormone replacement therapy.Another significant risk factor contributing to massive PLD is age. With age, liver cysts in individuals affected by the condition increase in number and size.In patients with PLD, the number and size of liver cysts grow with age, and the volume of the liver typically increases by nearly 2% every 6 to 12 months. Most patients affected by this disease, however, remain asymptomatic. Their liver function tests are usually normal because liver parenchyma is not entirely destroyed. Only a minority of PLD patients develop clinical symptoms. These patients, however, may become incapacitated by the disease due to massive hepatomegaly and experience severe abdominal pain, dyspnea, abdominal distention, early satiety, malnutrition, and regurgitation. Individuals with PLD may also present with cyst complications such as hemorrhage or infection, seriously affecting their quality of life. Moreover, due to the large mass of cysts in the liver, patients suffering from this disorder may develop vascular obstruction resulting in portal hypertension, ascites, splenomegaly, variceal bleeding, or encephalopathy.
LIVER SAGCTTRVUltrasound and CT images of the abdomen demonstrate massive liver enlargement with multiple prominent cysts throughout the hepatic parenchyma in a patient with PLD.46
he diagnosis of PLD is typically made when the number of liver cysts exceeds 20. The typical findings of isolated PLD on abdominal imaging include hepatomegaly and multiple liver cysts. When PLD occurs as an accompanying symptom of PKD, in addition to numerous liver cysts, innumerable bilateral renal cysts are typically evident.On ultrasound, liver cysts in patients suffering from PLD commonly appear as anechoic fluid-filled round spaces.Infection or intra-cystic hemorrhage is suspected if cysts have irregular thickening, internal septa, and debris. CT and MRI may be essential to assess PLD complications such as compression of the main portal vein and the mass effect of cysts on the inferior vena cava, biliary system, stomach, and diaphragm
Most PLD patients are asymptomatic and do not need any intervention. The treatment is typically reserved for a minority of patients with clinical symptoms caused by complications resulting from massive hepatomegaly, cyst rupture, infection, or bleeding. The main goal is to improve quality of life and minimize symptoms by reducing the progressive increase in cyst size.Up-to-date, there is no approved effective medical treatment for PLD. The most commonly used treatment options involve reducing the bulk of the cystic liver with percutaneous or surgical approaches. The first treatment option is usually abdominal percutaneous puncture and catheter insertion into the liver cyst with subsequent fluid drainage and injection of the sclerosing agent such as ethanol to destroy the epithelial lining of the cyst wall. This procedure often provides temporary relief; however, the cyst recurrence rate is high
The next treatment option for patients who have failed the first approach is cyst fenestration. This surgical procedure involves cutting windows into the cyst during laparoscopy, and draining the fluid into the peritoneal space, which gets absorbed by the peritoneal lining. After cyst fenestration, symptoms are greatly relieved in over 90% of cases. Unfortunately, a large number of patients suffer symptomatic recurrence and need reintervention.The next steps for treatment options involve either liver resection or liver transplantation. These are the last resort procedures; they are reserved for individuals with the most symptomatic disease or those who have failed the other treatment options. Resection has several associated complications, including significant morbidity and even mortality.Liver transplantation is the only cure for PLD; however, it is technically challenging in these patients due to the massive size of the liver and distortion of usual anatomic landmarks.The early mortality rate ranges from 10% to 20%, though once patients recover from the immediate postoperative period (approximately three months), their long-term survival after transplantation is excellent.51-53






댓글