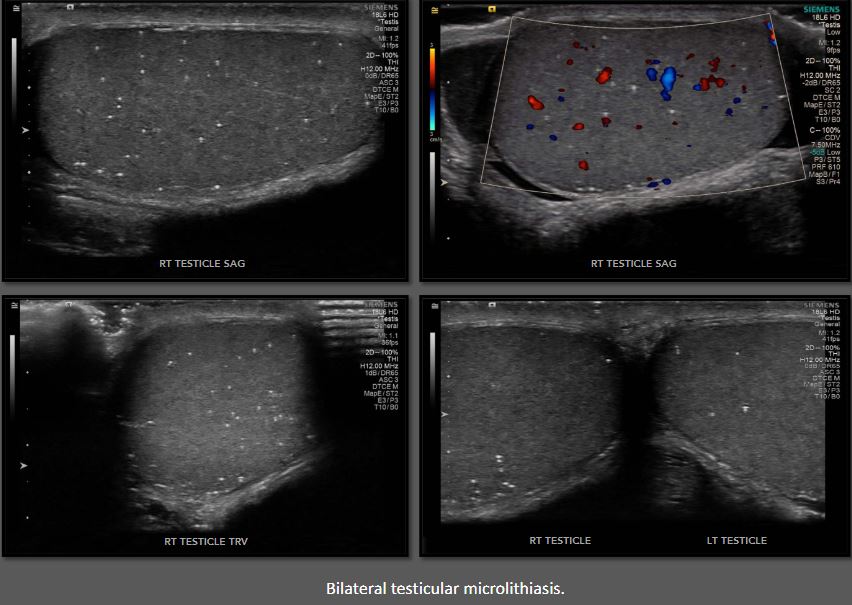
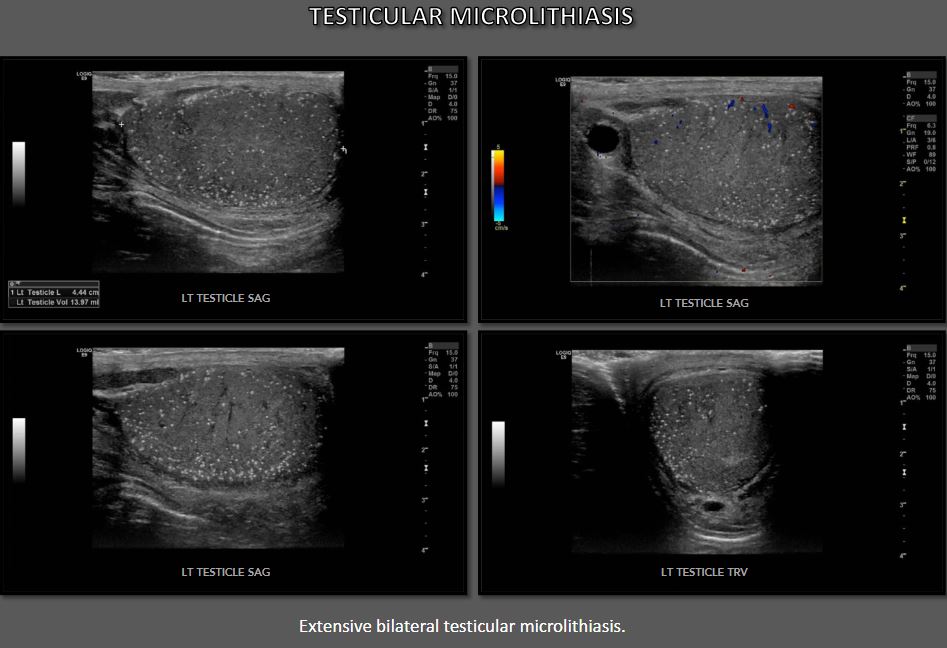
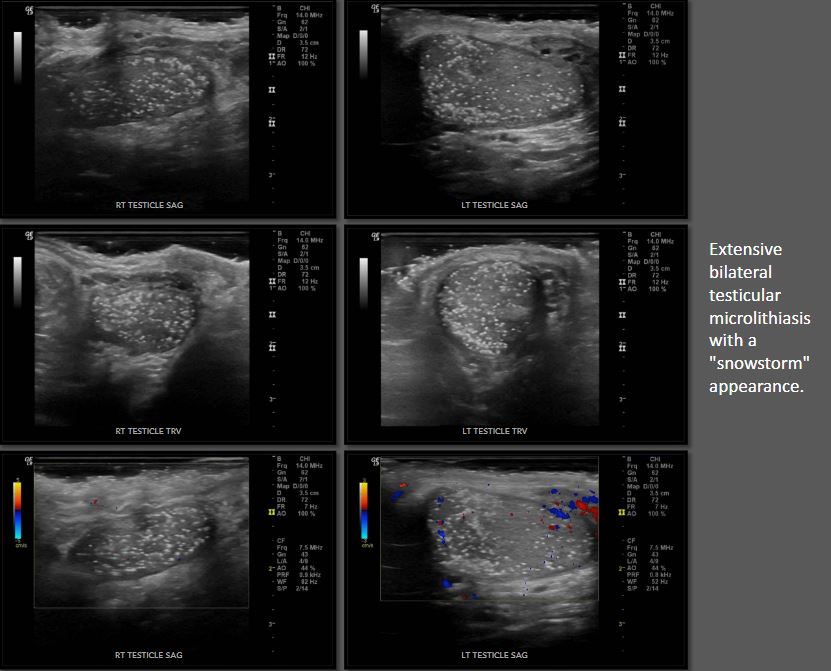
he first sonographic description is recorded in 1987 as "innumerable tiny bright echoes diffusely and uniformly scattered throughout in the substance of testes." Since then, a large number of varying descriptions and definitions have been used to establish the diagnosis of testicular microlithiasis. The most universally accepted definition involves five or more microliths seen per any single field of view (image) on ultrasound. Microliths associated with the condition present as small, same-sized (<3mm) echogenic foci without posterior shadowing observed throughout the testicles. Although the classic sonographic presentation of testicular microlithiasis is diffuse, microliths limited to only part of the testis have been reported
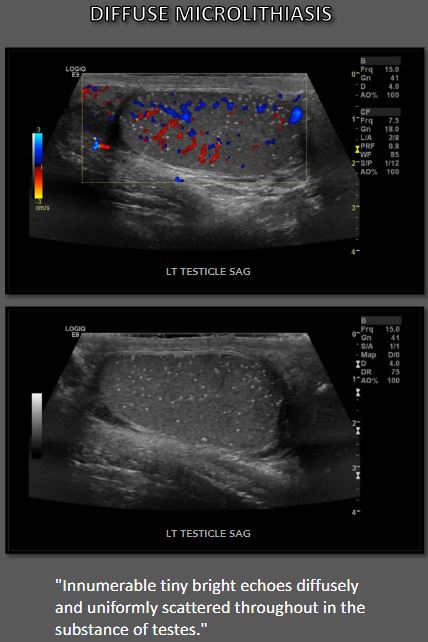
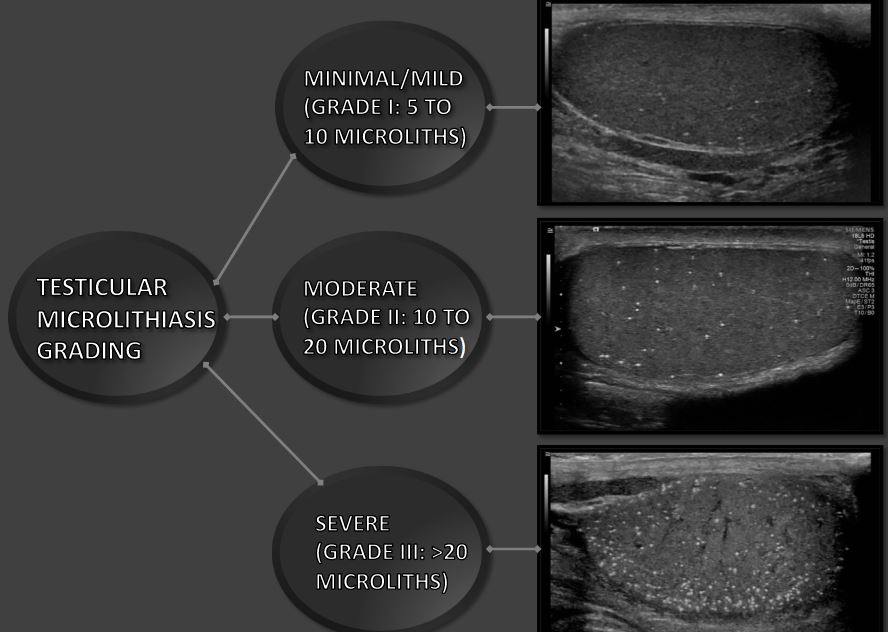
A twinkling artifact may be seen when assessing testicular microlithiasis with Color Doppler ultrasound. The number of microliths detected on imaging may vary considerably. The condition has been graded as minimal/mild (Grade I: 5 to 10 microliths), moderate (Grade II: 10 to 20 microliths), and severe (Grade III: >20 microliths) depending on the count of microcalcifications seen in any single view.

esticular microlithiasis affects males of all age groups, ranging from childhood to old age. Although the presentation is typically bilateral, the occurrence of unilateral cases is mentioned in literature. The microliths generally are asymptomatic; they do not cause pain and are too small to palpate. The etiology of the condition is unknown. Multiple theories have been put forward in an attempt to explain the origin. One such theory suggests genetic mutation as a possible cause. The prevalence of testicular microlithiasis in the general population is also unknown, primarily due to the asymptomatic nature of the condition.
here is an interesting study published in 2017 on the prevalence of testicular microlithiasis in relation to socioeconomic status and ethnicity of the affected patients. Black men were found to have a higher prevalence of the condition compared with white men. Another interesting finding of the study was that men from the most deprived socioeconomic groups had a significantly higher prevalence of testicular microlithiasis compared to men in the most affluent groups. Results of the study point towards ethnicity and lifestyle as possible influencing factors in the etiology of the condition.
Another study worth mentioning presented data showing that men with testicular microlithiasis reported significantly less physical exercise than men without microliths. Exposure to maternal smoking in utero has also been linked with an increased prevalence of the abnormality. Despite multiple attempts to decipher the nature of the condition, however, the precise etiology and prevalence of testicular microlithiasis remain an enigma
Multiple studies have reported an association between testicular microlithiasis and male-factor infertility; however, the relationship between the two conditions is not well understood. The indirect evidence suggests that testicular microlithiasis is linked with decreased fertility, and the extent of microlithiasis correlates inversely with semen parameters. Theoretically, men with testicular microlithiasis may have significant reductions in sperm migrations and motility due to the obstruction of seminiferous tubules by microcalcifications. However, some authors have reported no significant differences in sperm quality and function between infertile men with or without the condition. More research is needed to elucidate whether the conditions tend to co-occur or whether testicular microlithiasis directly contributes to the etiopathogenesis of infertility.
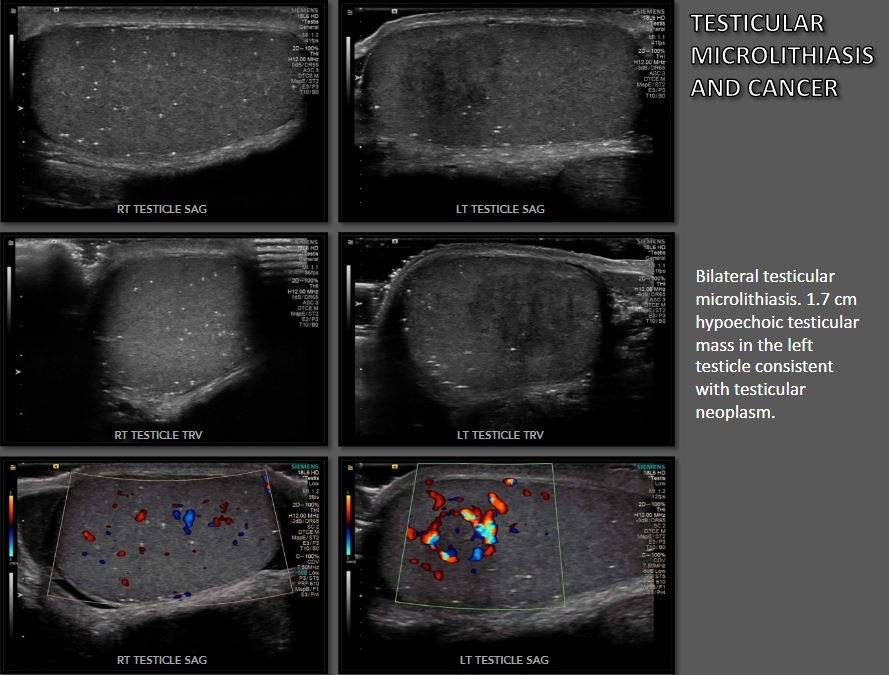
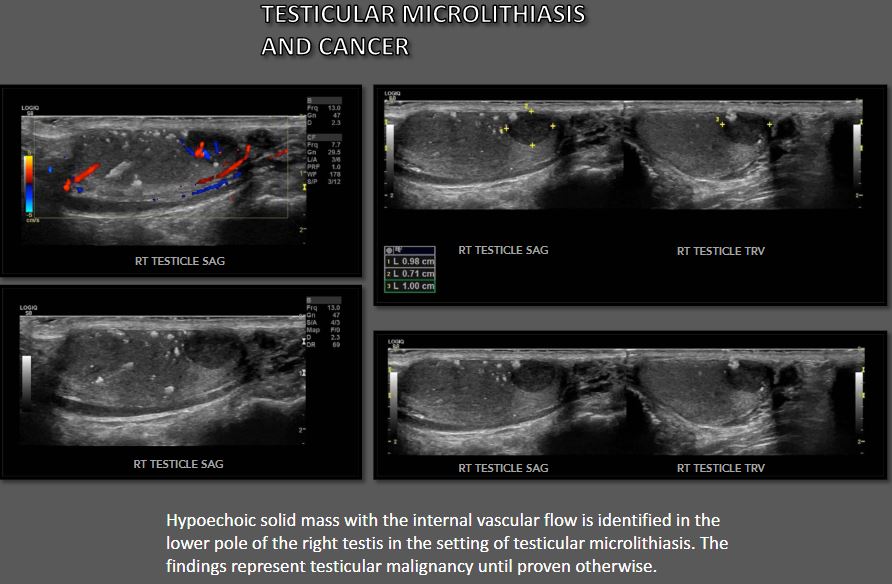
Testicular microlithiasis is not considered a malignant condition. This abnormality has been found in association with several nonneoplastic disorders such as testicular torsion, epididymitis, and cryptorchidism. Some authors, nevertheless, suggest that testicular microlithiasis should be regarded as a visible sign of a premalignant condition since there is also an association with testicular cancer. Indeed, in patients with a sonographically detected testicular cancer, there is a high rate of coexistent testicular microlithiasis. However, the relationship between the two conditions is unclear. There are inconsistencies with the theory of testicular microlithiasis being a risk factor for testicular cancer. For example, if testicular microlithiasis is an independent risk factor for testicular tumors, then there should be an increased incidence of testicular cancer in populations with a higher prevalence of testicular microlithiasis
In the United States of America, the rate of testicular microlithiasis is highest in the Southeast. However, the incidence of testicular cancer in that region compared with the rest of the country is the lowest.Furthermore, black men have a higher prevalence of testicular microlithiasis compared with white men. But testicular cancer is 5 times less common among the black population than among white people. This discrepancy calls into question a causal connection between testicular microlithiasis and testicular cancer. Up to date, it remains unclear whether testicular microlithiasis represents a cause, effect, or a common predisposing factor to testicular cancer.

there is no known cure for testicular microlithiasis. Depending on the patient's history and whether the condition is an isolated finding, suggested management approaches range from the clinical and sonographic follow-up to biopsy, looking for occult malignancy. More data is needed to establish the degree of risk (if any) isolated testicular microlithiasis poses to patients.
'on the wavelength > abdomen' 카테고리의 다른 글
| Lipoma/painless palpable mass/soft-tissue tumor (0) | 2023.04.16 |
|---|---|
| accessory spleen/Splenule (0) | 2023.04.15 |
| Duplication of gallbladder/cholecystectomy/ (0) | 2023.04.15 |
| biliary stone /Choledocholithiasis/CBD stone /sono (0) | 2023.04.15 |
| Liver cirrhosis ultrasound /portal hypertension /pseudocirrhosis/ (0) | 2023.04.14 |



댓글